CORNEA
What is a Cornea?The cornea is the outermost part of the eye. It is made of many layers of thin cells. It is clear, as a result we are not able to see it. The first structure of the eye we perceive is the iris which is the colored area: brown, blue, or green are the normal shades.
The cornea is masterfully crafted, naturally. Even the most expensive man-made lenses cannot match its precision of function and also self-preservation. The smoothness and shape of the cornea is critically important to its correct functioning as well its transparency. If either the surface degree of smoothness or the quality of the cornea is altered, vision will come to be compromised.
Although appearing to be one clear membrane, the cornea is composed of five distinctive layers of tissue, each with its own function. The thin outer layer, or epithelium, is a dependable challenge to corneal infection. It normally has to be damaged before any contagious bacteria or virus can enter between the layers of the cornea. Just below this layer is a fibrous band called Bowman’s membrane layer. It is important for the integrity of the cornea.
The third layer called the stroma is constructed from collagen, a connective tissue. This forms eighty percent of the cornea. Besides collagen fibrils, there are cells called keratocytes. The density of the fibers is higher towards the Bowman’s membrane. Below the stroma is again a fibrous layer. This is called Descemet’s membrane. It is the structure for the innermost layer of cells called Endothelium cells.
When endothelial cells are healthy and balanced, they work as a “pump-leak system” to provide nutrients to the cornea. In other words, these cells are nourishing and facilitate fluid from inside the eye (liquid food) to leak into the cornea. After the corneal cells have been nourished, these cells pump out the fluid from the cornea.
If the endothelial pump is compromised for any reason, the cornea will over hydrate and became hazy. This most often occurs in people that have suffered injury to the endothelial layer throughout complex cataract procedure or patients that have gotten a disease of the corneal endothelium described as Fuchs’ Endothelial Dystrophy.
A corneal transplant works like replacing the windshield of a car. When we drive at different times of the day, we need to be able to see through the windscreen out into the distance. The windscreen requires to be clear at all times. Dust or rain can hinder our capacity to see through it. Similarly, the cornea has to be always kept clear.
Light travels through the clear cornea on its course towards the retina in the back part of the eye. A healthy, balanced and clear cornea is required for perfectly clear vision. Occasionally, the cornea is described as the” window” to the eye. Occasionally, either through disease or injury, the corneal tissue is harmed to a point where light can no longer effectively pass through it, causing lowered vision.
Cornea Transplant or Corneal Transplantation?
Corneal transplant is the removal of the infected cornea of a person and changing it with a new cornea from a benevolent deceased person.
There are a large number of patients that struggle with a diseased or cloudy cornea. When this specific area of the eye starts to have trouble, light cannot pass through this area successfully, which leads to blurry vision or even loss of sight. When this happens, it depends on your ophthalmologist or an eye doctor to determine the best treatment for your particular problem. Currently, it’s important to understand that simply because the cornea is having a problem, before a corneal transplant can occur, it will need to be determined that the retina as well as the nerve at the back of the eye is entirely healthy and balanced.
Indicators for Cornea Transplant
Any kind of thick scarring or opacity in the cornea. This affects the vision and cannot be improved with glasses or contact lenses. We can categorize the reasons:
1. Genetic – Opacity like Peters anamoly.
2. Degenerative – Keratoconus, Macular corneal degeneration, Fuchs dystrophy
3. Trauma – Like central corneal injury
4. Tumors – Keloid
5. Pterygium which invades the central cornea
6. Post-surgical – Pseudophakic Bullous Keratopathy
Once this has been determined, your doctor can decide whether or not this is the proper technique that will need to take place. Now, corneal transplant is exactly what it sounds like. Your cornea is being transplanted with a new donated cornea. If you have been diagnosed correctly, and it has been decided that a transplant technique will work in your specific case, this is an alternative you will have – provided the new donated cornea is available.
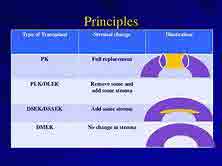
Types of Cornea Transplant
1. Full thickness Corneal graft called Penetrating Keratoplasty or PK
2. Lamellar Keratoplasty or LK
3. DALK or Deep Anterior Lamellar Keratoplasty
4. DSEK or Descemets Stripping Endothelial Keratoplasty
5. DMEK or Descemet Membrane Endothelial Keratoplasty
6. DWEK OR DSO– Descemets membrane stripping
Conventionally, manual keratomes have been used. We have now started using femtosecond lasers to get better shape alignments. This helps in enhancing wound apposition, strength as well as at the same time decreasing inducing astigmatism.
The exact type of cornea transplant best suited for you can be identified by a corneal cosmetic surgeon like Rajesh Khanna, MD based in the Los Angeles area. Call him at (310) 482 1240 if you need to find what is BEST for you.
Why choose a Cornea Transplant?
There are many patients that will wonder why they must pick a corneal transplant rather than any other kind of strategy available. Well, this is a question that can only be addressed when it comes to your specific situation. It is essential to understand that everyone is different and every one will suffer with a different type of eye problem. Each condition will not require this type of technique. Nonetheless, you’ll be happy to know that if you have been diagnosed thoroughly, and they find that this is a technique that can be used in your specific situation, you can benefit a great deal by having this procedure performed.
The Benefits of Corneal Transplantation
Among the significant benefits of corneal transplantation will be the fact that you can see again. However, it is very important to keep in mind that you will need to spend some healing time, but if all of the diagnostic procedures have been performed correctly, you’ll find that this is a procedure that takes really little time and when completed, you will be able to see again. It’s important to keep in mind that with any type of procedure available, there can be complications; nonetheless, 99.9% of the people that have been diagnosed for this technique have positively regained their sight to a significant degree.
So, when it comes to corneal transplantation, this is another option that is available for those that have been having corneal problems which are unresolved. As stated previously, it will be essential for you to work with your eye doctor or ophthalmolgist to figure out whether this is a technique that will provide you with great benefits.
Cornea transplant and Insurance policy Coverage
There are certain costs involved in a corneal transplant procedure. They can be divided into:
– Cost of the cornea from the eye bank
– Cost of the clinic
– Surgeon Fees
– Anesthetist Fees
– Laser Fees
– Preoperative measurements
– Follow up care
Normally medical insurance covers some or the most of the cost. Vision Insurance policy does not apply to this treatment Some insurances have stopped covering expenses for the Corneal graft. It is best to send us your medical insurance card beforehand, so we can examine your coverage.
Preparing for the Corneal Transplant procedure
A lot of arrangements are made by the surgeon, eye bank and the surgery center to procure the cornea and have it prepared for corneal transplant surgery. It is imperative, you do not try to reschedule the surgical procedure, unless it’s absolutely, medically necessary.
On the day of the surgical procedure, wear loose clothes. Do not drink or eat anything for eight hours before the scheduled time. You will have intravenous fluids and anesthetic given.
After the Cornea Transplant procedure.
You will be given certain important instructions as to how you should sleep, based upon the exact procedure. These need to be complied with, for effective outcomes.
DALK or Deep Anterior Lamellar Keratoplasty
What is DALK?
Deep Anterior Lamellar Keratoplasty. As the name suggests it is a type of keratoplasty or corneal transplant. There have been typically two kinds of replacement of cornea with a cadaver cornea. Full thickness graft referred to as Penetrating Keratoplasty or PK. The other type less commonly used was Lamellar keratoplasty or LK, this is a partial thickness cornea graft. Learn more about the Structure of Cornea.
DALK is a hybrid between LK and PK. It goes deep where no LK has ever before been before (language sounds like Star Trek, huh). It stops just short of the Descemets’ and endothelial layer.
Indications for the DALK procedure
DALK is indicated when the inner layers of the cornea are healthy but the superior layers have a pathology.
In Keratoconus eye disorder, the endothelium works but the collagen layer is weak. Keratoconus eye disease is present in younger patients. DALK is a great option for them. If the cornea has raptured, like in Hydrops, then DALK may not be possible.
Corneal Dystrophies and superficial scars, not treatable with PTK are great candidates for DALK. Scars may have varied etiology like post PRK scars, post traumatic or post infective. In case of herpetic scars, it is recommended to wait six months after the active infection has subsided.
Steps in DALK Surgery
1. Preparation of patients’ Cornea: The thickness of the host cornea is measured. Three fourths of this value is calculated. A corneal trephine is set to this thickness.
2. A needle is introduced through the trephined edge till it reaches the descemets membrane. An air bubble is introduced till it spreads uniformly across the cornea.
3. Lamellar breakdown is done with a crescent knife to eliminate the trephine surface cornea.
4. An air bubble is introduced into the anterior chamber. The constant presence suggests the endothelium has not been perforated.
5. The needle is reintroduced into the remaining cornea over the descemets membrane. A knife slits the remaining stroma of the cornea. This is than excised with corneal scissors.
6. The benefactor cornea graft, devoid of the inner layer is positioned on the bare descemets membrane layer as well as sutured with interrupted and/or continual stitches.
Advantage of DALK Transplant
1. Safer during surgical procedure as the eye is shut system. Consequently, the iris and also other content of the eye cannot come out.
2. The endothelium of the patient is maintained. The possibilities of endothelium being rejected are prevented.
3. Also, after DALK treatment, the eye is more resistant to injury.
4. Induced astigmatism is much less.
Disadvantages of DALK
1. It is technically harder to carry out
2. It may be necessary to convert it to PK on the operating table
3. The host donor junction can end up being hazy, affecting the best corrected vision.
Just what is DSEK or Descemet’s Stripping Endothelial Keratoplasty?
Some conditions of the cornea, however, simply affect the internal cellular lining of the cornea. A new variation of corneal transplant, known as a Descemet’s Stripping Endothelial Keratoplasty (DSEK), has been introduced as a new medical technique that utilizes simply an incredibly thin section of the cornea for transplant. DSEK is a partial corneal transplant strategy where the harmful, infected, posterior part of a person’s cornea is removed and replaced with a healthy slim corneal graft drawn from a dead body. Unlike Penetrating Keratoplasty (PK), the DSEK treatment uses only a partial density graft. As a result, it requires a much smaller sized surgical cut and also calls for no corneal stitches. This normally leads to extra fast visual rehabilitation for the patient and also decreases the risk of harmful issues that accompany the PK surgical procedure.
Indications for DSEK or Descemets Stripping Endothelial Keratoplasty
When the corneal endothelium is stressed out, the endothelial cells happen to be bigger and also much thinner. As endothelial cell numbers drop between 500 to 1000 cells/mm, the pump device can no longer protect a clear cornea. This may occur after extended complex cataract surgery. This entity is labelled as Pseudophakic Bullous Keratopathy.
When it comes to Fuchs’ dystrophy, the endothelial cells also start producing products that make Descemet’s layer thicker and non-transparent. Vision eventually degrades to a point where these patients seem like they are looking through wax paper. Such patients are ready prospects for the DSEK treatment.
Benefits of DSEK or Descemet’s Stripping Endothelial Keratoplasty
There are a lot of significant benefits of the DSEK procedure in comparison to the usual corneal transplant procedure.
1. In PK, there is a time when the eye is entirely open. If the patient were to stress or cough, the interior structure of the eye can prolapse forward. In hypertensive patients, there is also the possibility, the retina might come out. This is called expulsive hemorrhage. In DSEK only a small cut, similar to that used in cataract eye surgery is made.
2. There are several stitches made use of in PK or Penetrating keratoplasty. DSEK or Descemets Stripping Endothelial Keratoplasty is either stich-less or one or two stitches might be called for
3. The possibilities of being rejected are much less in DSEK
4. The induced Astigmatism in PK is high compared to the practically negligible amount in DSEK
5. Integrity of the eye is much better in DSEK than in PK
6. Returning to an active lifestyle and resumption of work is faster with DSEK
The recovery with PK can be rather long, as much as twelve months. It is also not unusual to have significant irregular curvature of the cornea as an outcome of the stitches. In most cases, a prescription lens is required to attain the very best vision. Ultimately, a full density corneal transplant can have continued weakness, years later, such that a small trauma can disarrange the graft from its setting. Cornea experts have done DSEK surgery for the previous 10 years with amazing success. Future endothelial transplant research will center on making the procedure much more trusted and also not as surgeon-dependent.
Steps of Descemet’s Stripping Endothelial Keratoplasty
The transplant tissue can be made manually by the corneal surgeons in the operating suite. This is done utilizing a special punch and fine dissection. There is a chance of harming the graft as it is an extremely delicate procedure. The trend has been to buy premade graft from the eye-bank. Service technicians there do a multitude of graft harvesting so they end up being adept at the treatment. Additionally, if the graft is damaged, they can make use of one more donor cornea to yield the graft.
In the event the patient elects to have the surgery, the doctor is going to have the patient authorize an informed consent. You’re going to be awake during the process and also the majority of patients do not report any type of pain. Dr. Khanna consistently performs this treatment simply utilizing eye drops to numb the eye. Some people might be offered local or general anesthetic, especially if their general medical condition is in question.
The DSEK procedure takes about 45 minutes to 1 hour. After the eye is prepared and curtained in sterilized drapes, an eye retainer is put to keep the eyelids open. The Cornea surgeon removes the harmful inner cell layer of the cornea. The surgeon implants healthy donor tissue through a little cut. Dr. Khanna then uses an air bubble to unfold and position the donor tissue against the patient’s cornea. The small cut is either self-sealing or might be closed with a stitch or more.
A lot of patients have minimum pain after surgical treatment. The patient is asked to lie straight in the healing area for about 45 minutes to an hour and is seen once more before being discharged. For the preliminary 24-hours after surgery, patients are requested to rest on their back with their face pointed straight at the ceiling for as much time as they can endure. They begin to see once the bubble liquifies over the succeeding 2-3 days. They can go back to regular work, a week or two after surgery.
Alternatives to DSEK or Descemets Stripping Endothelial Keratoplasty
Given that damaged or marked corneal tissue do not permit light to effectively fall on the eye and reach the retina, poor vision and blindness might occur from a damaged cornea. Patients with a stromal mark rather than endothelial dysfunction will require a penetrating keratoplasty as opposed to a DSEK or Descemets Stripping Endothelial Keratoplasty.
Full Thickness Penetrating Keratoplasty and Lamellar Thickness Keratoplasty have come before DSEK. One newer treatment where only Descemet’s is removed is called DWEK. It has just restricted indicators in specific Fuchs patients. ROCK inhibitors need to be utilized.
Much more preferred and also a finer procedure is DMEK. Here as shown the picture, an even thinner graft is utilized. The graft here is one tenth the thickness of DSEK.
Disadvantages of DSEK Technique
A problem that could occur from the DSEK treatment that is not connected with a standard transplant is a graft displacement, where the round disc slips from its desired positioning. In this condition, the donor disc needs to be repositioned in the operating area. If the air bubble escapes, the graft might get displaced, needing one more air bubble. The interface between the host and donor is not completely smooth. This might limit vision in a few patients. DSEK also adds more tissue than it gets rid of. It might result in a hyperopic shift.
Below is a DSEK eye surgical procedure video.
When looking for a Los Angeles DSEK or Descemets Stripping Endothelial Keratoplasty surgeon it is necessary to pick a person with superior understanding in issues linked to the cornea. Your cornea surgeon should have the ability to choose whether a DSEK partial cornea transplant is the perfect procedure for you.
DMEK or Descemet’s Membrane Endothelial Keratoplasty
DMEK or Descemet’s Membrane Endothelial Keratoplasty is the contemporary development in corneal transplant surgery. It is a more recent variant of DSEK corneal surgery. It entails transplanting only the internal 15 microns of the cornea.
Indications for DMEK
It is indicated in Fuchs dystrophy, Pseudophakic Bullous Keratopathy and also other corneal disease limited to the innermost lining of the cornea. A requirement is that, the remaining cornea should be healthy. If there is opacity in the center of the cornea, then a full thickness graft might be more appropriate. Managing this ultra-thin graft needs a high level of dexterity. This behooves a clear view beneath the cornea. The upper layer of the cornea called the epithelium can be removed to increase clarity.
The DMEK treatment
The treatment includes 3 parts. Collecting the graft from the donor, the cornea is the primary step. Next the recipient cornea is prepared to receive the graft. Lastly, the endothelial graft is introduced into the patient,s eye and also made to follow the cornea.
STEP 1 OF DMEK
The donor cornea is placed endothelial side up in a punch like a Moria disposable punch. A plain instrument is made use of to separate the descemets from the schwalbes’ line. When roughly 60 percent has actually been cleaved, the corneal switch is centered over 4 holes. It is then dyed with trypan blue. It is then punched with a 7.5 mm to 8 mm trephine. The descemets is divided from the rest of the cornea. It is soaked in trypan blue and covered. Attention is then directed to the patient.
Nowadays, doctors like to get a precut preloaded ready graft. This graft, now has a mark to identify its orientation.
STEP 2 OF DMEK PROCEDURE
The patient’s eye is prepped as well as draped. Some surgeons proceed with topical anesthetic drops. Others like to execute a retrobulbar block to prevent eye movement. A speculum is inserted. The center of the cornea is identified. A ring of 8mm is put over it. The indentations are marked with a marking pen. Two 1 mm paracentesis lacerations are made. Viscoelastic is injected in the eye. The primary temporal cut is 3 to 5 mm. A reverse sinksy instrument scores the descemets’ and endothelium along the pre-inked corneal marks. This tissue is then stripped off. A forceps gets it. It is then placed over the cornea to verify it is uniform. Also, the inner cornea is checked to identify if there are any kind of strips of the tissue left behind. An opening is made in the iris at 6 or 9 o’clock. If all is great, the viscoelastic is gotten rid of. Any residual viscoelastic is an enemy to the donor graft, states Dr. Khanna.
Step 3 of DMEK
Now is the most tough part. The graft is filled into a specifically developed round glass device affixed to a syringe. For this reason, the graft gets curled with the endothelial side up. This tool is introduced into the temporal cut. With gentle presses, the graft is pressed into the anterior chamber of the eye. Then the dancing starts, as we desire the graft to unravel. The cornea is gently touched as well as rolling motions performed. An air bubble is introduced under the flap, once it opens. The said S or F is determined to verify, it is ideal side up. Air is presented to increase the pressure of the eye for next 10 minutes. Then a little of the air is released. A subconjunctival injection of steroid and anti-biotics is offered.
Patient is moved, but made to lie level on their back for the following hour. They are also instructed to do the very same in their home.
DWEK or DSO is a sort of Corneal graft
Well, in a recent post we discussed DSEK and DMEK. These are options to full density penetrating corneal grafts. They may also be called suture-less corneal grafts.
Now one of the doctors whose DMEK graft fell off, found out the cornea still recovered. The understanding dawned that removing simply the infected endothelium might be all that is called for in particular patients. This treatment is called DWEK or DSO. DWEK stands for Descemets stripping without Endothelial Keratoplasty. An even more apt name might be DSO Descemets removal only.
This is revealed to work in a couple of selected patients. The very best candidate may be an older person with simply central thick Fuchs guttate. Central 4 mm of endothelium is removed. The adjoining healthy cells migrate and also take control of the function of the unwanted cells. The cornea clears and vision improves. This process can take 3-4 months.
DMEK clears up the cornea quicker and is preferred in younger patients. DSEK is the initial treatment which entailed removal of the unfit inner corneal tissue. Really, all these surgical interventions are a continuum of internal corneal transplants. The difference being just how much of the infected cornea is removed. And whether a transplant is done. If removed, then the thickness might vary.